
I Never Knew Lobular Breast Cancer Existed — Until I Became the Patient
I still remember sitting in my office after a long shift, thinking how I, as a nurse, knew so much about health — and yet I felt completely unprepared the day I became the patient. My name is Tammy McDevitt, I’m 63 years old, and for most of my life, I thought breast cancer was one disease. You found a lump, got a scan, started treatment — that was it. But when I was diagnosed with invasive lobular breast cancer, I learned how quietly it can hide, how “sneaky” it truly is, and how easily it can go unnoticed until it’s far more advanced than anyone realizes.

I’ve been a registered nurse care coordinator at the Cleveland Clinic’s Neurological Institute for years, and I’ve seen my share of medical stories. But I never thought I’d live one like this. For a long time, my mammograms came back clean, even though I was always told I had dense breast tissue — something that makes it harder for traditional imaging to spot small abnormalities. Every time I got that letter saying “normal,” I felt relief. But I also remember thinking, maybe they’d never find something if it really were there.

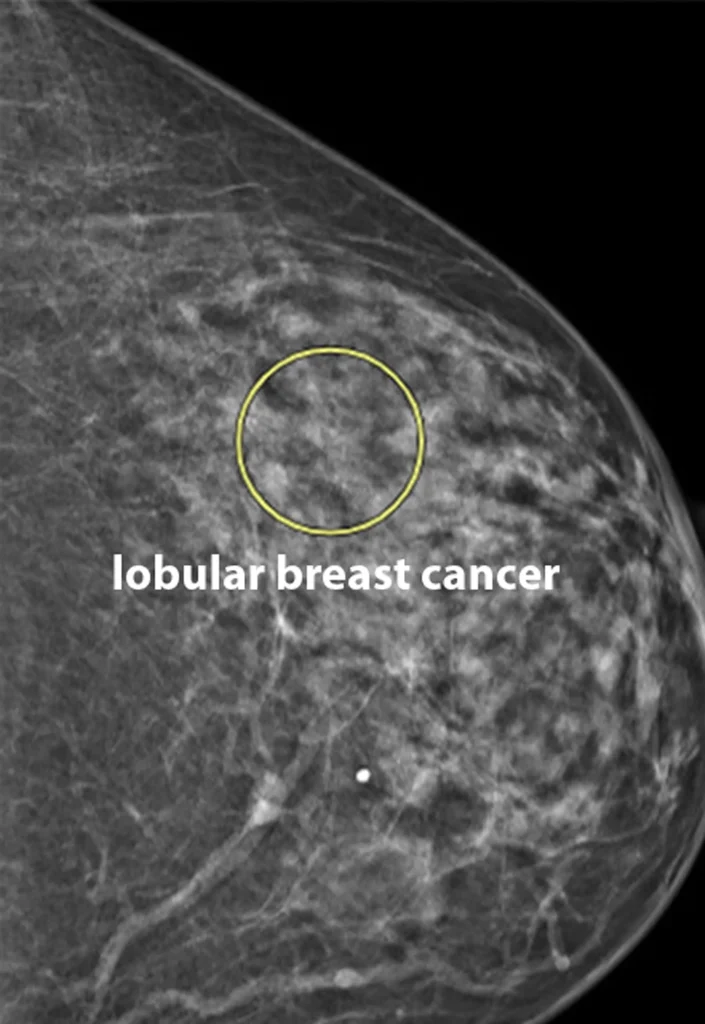
Then came the day that changed everything. My latest mammogram showed what doctors called an “architectural distortion” in my left breast. It wasn’t a lump — just a tiny, twisted shift in the pattern of tissue. The kind of detail you might miss if you blink. I was called back for another scan, then a biopsy. When the results came in, I heard the words no one ever wants to hear: it’s malignant. That was the day I went from being a nurse to being a patient.

I was shocked to learn how different lobular breast cancer is from the more common ductal type. It doesn’t usually form solid lumps. Instead, it spreads in thin, web-like patterns that don’t always show up on imaging until later stages. That’s why doctors sometimes call it “the sneaky cancer.” Knowing I could’ve missed it for another year still chills me.

After my diagnosis, the treatment plan moved fast. I had a partial mastectomy and reconstruction, followed by radiation therapy. Thankfully, I didn’t need chemotherapy, but I do take a hormone-blocking medication every day for the next ten years to prevent recurrence. My cancer was hormone-receptor positive, which means it feeds on estrogen, so my doctors wanted to make sure they cut off that fuel completely.
As a nurse, I always believed knowledge was power. But going through this myself gave me something deeper — empathy. Now when I talk to my patients, I understand the fear in their voices, the exhaustion in their eyes. I know what it’s like to wait for test results, to hold your breath when the phone rings. It’s changed how I care for people forever.

There’s also a strong family history I can’t ignore. My mother had breast cancer, and my aunt died of ovarian cancer. I tested negative for the BRCA gene mutation, but that doesn’t erase the worry. I think of my daughter often and remind her to stay vigilant, to never delay a screening or dismiss a small change in her body.

Faith and family carried me through the hardest days. My friends from work brought food, my grandchildren made cards, and every text, every prayer reminded me I wasn’t alone. There were tears, yes — but also gratitude. I’m still here. I’m still able to live, laugh, work, and share my story.

I’ve come to see that sharing my experience is its own kind of nursing. If one woman hears this story and decides to schedule her mammogram, then it’s all been worth it. Lobular breast cancer accounts for around 15 to 20 percent of all invasive breast cancers — but it’s still one many people haven’t heard of. And that’s what makes it dangerous.
So please, if you’re reading this, listen to your body. Don’t wait. Don’t skip your yearly exam. Sometimes the most important thing you can do for yourself is show up — even when you think you’re fine. Because early detection doesn’t just save lives — it saved mine.


